Tirzepatide 5mg
$250.00
Tirzepatide is a synthetic derivative of gastric inhibitory polypeptide (GIP) that has simultaneous glucagon-like peptide-1 (GLP-1) functionality as well. This combination allows Tirzepatide to lower blood glucose levels, increase insulin sensitivity, boost feelings of satiety, and accelerate weight loss. Tirzepatide was developed to fight type 2 diabetes, but has additionally been shown to protect the cardiovascular system and act as a potent weight loss agent.
Product description
Tirzepatide
Tirzepatide is a synthetic analogue of gastric inhibitory polypeptide (GIP) that was developed for its ability to stimulate insulin release and thus address both type 2 diabetes and non-alcoholic fatty liver disease. Made up of 39 amino acids, the relatively large Tirzepatide stimulates the release of insulin from the pancreas by binding to both GIP and GLP-1 (glucagon-like peptide-1) receptors. Taken over longer periods of time, Tirzepatide increases adiponectin levels by as much as 26% as well[1]. Research shows that Tirzepatide reduces feelings of hunger, lowers insulin levels, and increases insulin sensitivity increases insulin sensitivity. Taken together aken together, these ef , these effects cause significant weight loss of 1 fects cause significant weight loss of 11 kg (25 lbs), improve glucose tolerance, decrease fat (adipose) tissue, and reduce cardiovascular risk.
Tirzepatide Structure
Amino Acid Sequence: YE-Aib-GTFTSDYSI-Aib-LDKIAQ (C20 fatty
acid) AFVQWLIAGGPSSGAPPPS
Note: Aib is a non-coded (non-proteinogenic) amino acid – H2H-C(CH3
)2
-COOH
Molecular Formula: C225H348N48O68
Molecular Weight: 4813.527 g/mol
PubChem CID: 156588324
CAS Number: 2023788-19-2
Synonyms: P1206, LY3298176
")
What Does Tirzepatide Do?
Simply put, Tirzepatide increases the release of insulin from the pancreas resulting in improved glucose control. Research shows that, in individuals with Type 2 diabetes, Tirzepatide decreases hemoglobin A1c (HbA1c) levels by 2.4% after six months. The peptide also appears to aid in weight loss, showing a dose-dependent relationship and helping individuals lose as much as 11 kg (25 lbs) over six months[1], [2]. It isn’t just that Tirzepatide increases insulin release though. Research suggests that the peptide actually improves the function of pancreatic beta cells, the cells that make and release insulin. Studies suggest that Tirzepatide may actually make beta cells more effective at processing insulin, which leads not just to increases in insulin levels in the bloodstream, but decreased stress on the beta cells themselves. This may, in turn, help to slow the progressive nature of type 2 diabetes.
Research shows that Tirzepatide doesn’t just increase insulin levels at random though. It appears to do so only in response to increased blood glucose levels. During fasting, Tirzepatide actually decreases insulin levels and thus helps to increase insulin sensitivity over time. It also decreases fasting levels of glucagon, which are thought to exacerbate hyperglycemia by interfering with hepatic glucose metabolism. Overall, these changes are a big part of the reason Tirzepatide has a profound effect on glucose and, ultimately, HbA1c levels[3].
How Does Tirzepatide Work?
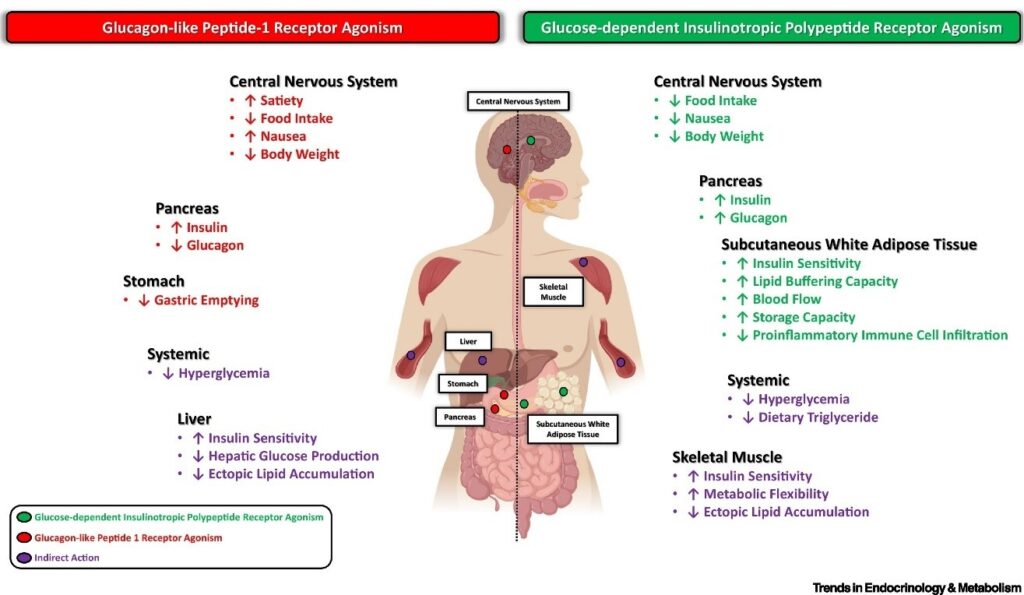
Tirzepatide is a dual agonist of the gastric inhibitory polypeptide receptor and the glucagon-like peptide-1 receptor. Action at these receptors appears to have synergistic effects that make Tirzepatide more effective than strict GLP-1 agonists that are already approved for the treatment of type 2 diabetes. of type 2 diabetes. The affinity of finity of Tirzepatide for the GIP irzepatide for the GIP receptor is greater than its af receptor is greater than its affinity for the finity for the GLP-1 receptor. Gastric inhibitory polypeptide, which is also referred to as the glucose-dependent insulinotropic polypeptide, is synthesized naturally in the small intestine. This polypeptide binds to the GIP receptor to inhibit gastric acid secretion and gastrin release while stimulating insulin release. The latter is the primary function of GIP-R and is the primary reason that insulin levels increase following a meal. Glucagon-like peptide-1 receptors are found on beta cells as well as in neurons in the brain. Like GIP-R, stimulation of GLP-1R stimulates the release of insulin. Natural agonists include glucagon and GLP1, but it has also been shown to bind nearly a dozen synthetic agonists including dulaglutide, lithium, and oxyntomodulin. Activation of GLP-1R increases both insulin synthesis and insulin release, factors that have made it a desirable target in drug development. In the brain, GLP-1R stimulation lowers appetite. Interestingly, stimulation of GLP-1R appears to increase beta cell density in the pancreas. GLP1R stimulation increases expression of the anti-apoptotic bcl-2 gene while reducing expression of pro-apoptotic bax and caspase-3 genes. This leads to enhanced beta cell survival and, ultimately, to increased levels of insulin[4]. The combination of GIPR and GLP-1R activity is what gives Tirzepatide an edge over strict GLP1R agonists. Research shows that Tirzepatide acts identically to GIP at the GIPR, but favors cAMP production over β-arrestin recruitment when acting at the GLP-1R. These details may seem esoteric to some extent, but this difference in activity from endogenous GLP-1 appears to cause GLP-1R activation without increasing physiological internalization of the receptor. The net result is enhanced GLP-1R activity with Tirzepatide compared to both endogenous GLP-1 as well as other synthetic GLP-1R agonists[5]. These slight alterations mean that Tirzepatide drastically enhances insulin secretion, promotes feelings of satiety, and reduces inflammation in adipose tissue. These combined effects make it a highly efficacious anti-diabetes peptide. Finally, Tirzepatide appears to alter adiponectin levels, raising overall levels of the fat-burning peptide. Increased levels of adiponectin reduce fat cell differentiation and increase energy expenditure by making mitochondria more inefficient. A low level of this peptide hormone has been implicated in diseases such as type 2 diabetes, atherosclerosis, and non-alcoholic fatty liver disease[6]. It is worth noting that elevated adiponectin levels elevate insulin sensitivity, so it would appear that Tirzepatide modulates insulin sensitivity via several mechanisms.
Tirzepatide and Hunger
Research shows that Tirzepatide delays gastric emptying during the earliest phases of its administration but that the effect diminishes over time as a result of tachyphylaxis[7]. These effects are similar to those seen with pure GLP-1R agonists, indicating that this action of Tirzepatide is almost completely controlled by its GLP-1 activity and not at all by its GIP activity. It appears that the effects of Tirzepatide on gastric emptying can be prolonged if the peptide is taken at a low dose for four weeks and then the dose is escalated. This also helps to mitigate side effects caused by the peptide and creates a veritable win-win for patients. Delayed gastric emptying can help to increase feelings of satiety and reduce hunger as well as food cravings. Combined with the effects Tirzepatide has on glucose levels, this can actually help to alter eating patterns over the long term.
Tirzepatide and Weight
As noted above, Tirzepatide use is associated with substantial weight loss over a six-month time interval. A comparison of Tirzepatide to other GLP-1 analogues, like degludoc, indicates a striking difference. Whereas Tirzepatide causes a dose-dependent decrease in weight over time, degludoc and other GLP-1R agonists cause weight gain[12]. It appears that the GIP agonism cause by Tirzepatide is what is responsible for the peptide’s longterm effects on weight. GIP appears to directly impact the insulin-sensitivity of adipocytes, which is likely the mechanism by which Tirzepatide impacts adiponectin levels. In short, Tirzepatide activates GIP receptors in fat cells, which then leads to an increase insulin sensitivity. This, in turn, leads to a reduction in adipose inflammation as well as an increase in adiponectin levels and the associated benefits. This isn’t the whole picture, however. Research shows that GIP signaling in the central nervous system regulates hypothalamic feeding centers leading to decreased food intake and improved glucose handling. This, in turn, leads to decreased body weight[13]. Thus, it appears that Tirzepatide impacts weight via adiponectin signaling directly in adipose tissue and via CNS alterations that reduce hunger levels via GIPR signaling in the brain
Tirzepatide and the Heart
As noted, Tirzepatide alters adiponectin levels. Low adiponectin has been associated with atherosclerosis, obesity, and heart disease while increased adiponectin levels have been associated with decrease risk of all of these things. Research in humans with type 2 diabetes has shown that Tirzepatide improves lipoprotein biomarkers, lowering levels of triglycerides, apoC-III, and a handful of other lipoproteins[8]. Combined, these effects mean reduced risk of heart disease as a likely result of decreased adiposity. Research shows that increased adiponectin levels increase HDL levels while decreasing triglyceride levels, both of which are associated with lower risk of heart disease. The peptide hormone appears to go further though, reducing scavenger receptors in macrophages and increasing the levels of cholesterol efflux to greatly protect against atherosclerosis. Increases in adiponectin levels have been associated with improved nutrition, exercise, and the use of certain lipid-lowering medications[9]. It appears that Tirzepatide has similar beneficial effects. Research shows that GLP-1 is important in both the direct regulation of cardiovascular risk factors such as hypertension, dyslipidemia, and obesity as well as in the indirect regulation of risk factors like inflammation and endothelial cell dysfunction[10]. The former effects are discussed above and below in relationship to adiponectin. The effects on inflammation and endothelial function, however, appear to be mediated more directly. In the case of endothelial function, GLP-1 signaling has been shown to induce relaxation of blood vessels leading to decreased blood pressure and enhanced end organ perfusion. This effect appears to result from increased expression of eNOS, the enzyme that generates nitric oxide and induces vascular relaxation. Interestingly, these effects appear to be enhanced in the setting of preexisting cardiovasulcar disease and diabetes[10]. Of course, it is well known that inflammation is directly correlated with atherosclerosis. The details are still being worked out, but GLP-1 signaling appears to decrease inflammation via a handful of mechanisms including reduced NF-κB signaling, decreased MMP-9 activity, inhibited inflammatory cytokine synthesis, and decreases in inflammatory macrophage activity. What is more, these effects appear to last as long as three months after a single dose of a GLP-1R agonist like Tirzepatide[10]. Tirzepatide is undergoing a clinical trial to further evaluate its medium-term effects on individuals with heart failure[11]
Tirzepatide Summary
Tirzepatide is a synthetic derivative of gastric inhibitory polypeptide (GIP) that has simultaneous glucagon-like peptide-1 (GLP-1) functionality as well. This combination allows Tirzepatide to lower blood glucose levels, increase insulin sensitivity, boost feelings of satiety, and accelerate weight loss. Tirzepatide was developed to fight type 2 diabetes, but has additionally been shown to protect the cardiovascular system and act as a potent weight loss agent.
Article Author
The above literature was researched, edited and organized by Dr. E. Logan, M.D. Dr. E. Logan holds a doctorate degree from Case Western Reserve University School of Medicine and a B.S. in molecular biology.
Scientific Journal Author
Dr. Kyle Sloop is a Research Advisor in the Endocrine Discovery Division of Lilly Research Laboratories at Eli Lilly and Company in Indianapolis. He received a B.Sc. in biology from Indiana University, a M.Sc. in biotechnology from Northwestern University, and the Ph.D. in molecular biology and biochemistry from Purdue University. Dr. Sloop’s research investigates molecular mechanisms that control glucose homeostasis, including insulin secretion and action, with a focus on novel therapeutic targets for metabolic disease. He leads interdisciplinary teams on early drug discovery effort, has formed alliance partnerships with external companies specialized in enabling technologies, and currently has established basic research collaborations with international investigators to explore mechanism of action studies for high value targets, including the areas of GPCR allosterism, ligand bias signaling, and protein-protein interaction. He previously served on the Research Affairs Committee of the Endocrine Society and as faculty for the Society’s Early Investigators Workshop and Early Career Forum. Dr. Kyle Sloop is being referenced as one of the leading scientists involved in the research and development of Cardiogen. In no way is this doctor/scientist endorsing or advocating the purchase, sale, or use of this product for any reason. There is no affiliation or relationship, implied or otherwise, between Peptide Sciences and this doctor. The purpose of citing the doctor is to acknowledge, recognize, and credit the exhaustive research and development efforts conducted by the scientists studying this peptide. Dr. Kyle Sloop is listed in [5] and [14] under the referenced citations
Reference
1. M. K. Thomas et al., “Dual GIP and GLP-1 Receptor Agonist Tirzepatide Improves Beta-cell Function and Insulin Sensitivity in Type 2 Diabetes,” J. Clin. Endocrinol. Metab., vol. 106, no. 2, pp. 388-396, Nov. 2020, doi: 10.1210/clinem/dgaa863.
2. T. Min and S. C. Bain, “The Role of Tirzepatide, Dual GIP and GLP-1 Receptor Agonist, in the Management of Type 2 Diabetes: The SURPASS Clinical Trials,” Diabetes Ther., vol. 12, no. 1, pp. 143–157, Jan. 2021, doi: 10.1007/s13300-020-00981-0.
3. Frias, Juan Pablo, et al. “Efficacy and Tolerability of Tirzepatide, a Dual Glucose-Dependent Insulinotropic Peptide and Glucagon-like Peptide-1 Receptor Agonist in Patients with Type 2 Diabetes: A 12-Week, Randomized, Double-Blind, Placebo-Controlled Study to Evaluate Different Dose-Escalation Regimens.” Diabetes, Obesity and Metabolism, vol. 22, no. 6, 11 Feb. 2020, pp. 938-946, 10.1111/dom.13979.
4. “Resurrecting the Beta Cell in Type 2 Diabetes,” Medscape. http://www.medscape.org/viewarticle/544820 (accessed Apr. 03, 2022).
5. F. S. Willard et al., “Tirzepatide is an imbalanced and biased dual GIP and GLP-1 receptor agonist,” JCI Insight, vol. 5, no. 17, p. e140532, doi: 10.1172/jci.insight.140532.
6. M. L. Hartman et al., “Effects of Novel Dual GIP and GLP-1 Receptor Agonist Tirzepatide on Biomarkers of Nonalcoholic Steatohepatitis in Patients With Type 2 Diabetes,” Diabetes Care, vol. 43, no. 6, pp. 1352-1355, Jun. 2020, doi: 10.2337/dc19-1892.
7. Urva, Shweta, et al. “The Novel Dual Glucose-Dependent Insulinotropic Polypeptide and Glucagon-like Peptide-1 (GLP-1) Receptor Agonist Tirzepatide Transiently Delays Gastric Emptying Similarly to Selective Long†Acting GLP-1 Receptor Agonists.” Diabetes, Obesity and Metabolism, vol. 22, no. 10, 13 July 2020, pp. 1886-1891, 10.1111/dom.14110.
8. Wilson, Jonathan M., et al. “The Dual Glucose-Dependent Insulinotropic Peptide and Glucagon-like Peptide-1 Receptor Agonist, Tirzepatide, Improves Lipoprotein Biomarkers Associated with Insulin Resistance and Cardiovascular Risk in Patients with Type 2 Diabetes.” Diabetes, Obesity and Metabolism, vol. 22, no. 12, 15 Sept. 2020, pp. 2451-2459, 10.1111/dom.14174.
9. H. Yanai and H. Yoshida, “Beneficial Effects of Adiponectin on Glucose and Lipid Metabolism and Atherosclerotic Progression: Mechanisms and Perspectives,” Int. J. Mol. Sci., vol. 20, no. 5, p. 1190, Mar. 2019, doi: 10.3390/ijms20051190. [
10. M. Tate, A. Chong, E. Robinson, B. D. Green, and D. J. Grieve, “Selective targeting of glucagon-like peptide-1 signalling as a novel therapeutic approach for cardiovascular disease in diabetes,” Br. J. Pharmacol., vol. 172, no. 3, pp. 721-736, Feb. 2015, doi: 10.1111/bph.12943.
11. UCSD, “UCSD Obesity Trial: A Study of Tirzepatide (LY3298176) in Participants With Heart Failure With Preserved Ejection Fraction and Obesity (SUMMIT).” https://clinicaltrials.ucsd.edu/trial/NCT04847557 (accessed Apr. 03, 2022).
12. B. Ludvik et al., “Once-weekly tirzepatide versus once-daily insulin degludec as add-on to metformin with or without SGLT2 inhibitors in patients with type 2 diabetes (SURPASS-3): a randomised, open-label, parallel-group, phase 3 trial,” Lancet Lond. Engl., vol. 398, no. 10300, pp. 583-598, Aug. 2021, doi: 10.1016/S0140-6736(21)01443-4.
13. Q. Zhang et al., “The glucose-dependent insulinotropic polypeptide (GIP) regulates body weight and food intake via CNS-GIPR signaling,” Cell Metab., vol. 33, no. 4, pp. 833-844.e5, Apr. 2021, doi: 10.1016/j.cmet.2021.01.015.
14. R. J. Samms, M. P. Coghlan, and K. W. Sloop, “How May GIP Enhance the Therapeutic Efficacy of GLP-1?,” Trends Endocrinol. Metab., vol. 31, no. 6, pp. 410-421, Jun. 2020, doi: 10.1016/j.tem.2020.02.006.
ALL ARTICLES AND PRODUCT INFORMATION PROVIDED ON THIS WEBSITE ARE RESEARCH PEPTIDES.
You may also like